In Coping with Nightmares 1, I’ve written a little about common causes of nightmares and how working on those directly can help. Here I’ve roughly grouped most of my own strategies, the suggestions of other people, or some ideas I’ve read into two different approaches; engaging with the nightmares, or working to reduce their impact. You may find one of these approaches more effective than the other, you may find that some ideas are no help at all to you, or it may be that combining both approaches works best for you. Sometimes it’s not that one approach is or isn’t helpful for you, but getting the timing right, or alternating strategies so you don’t unbalance. I describe this process of picking up and putting down emotionally charged material more here.
Engaging with Nightmares:
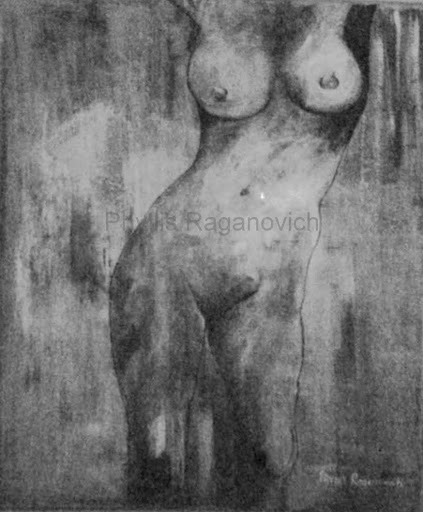
Sometimes the most effective way to help your mind stop sending you nightmares is to engage with the content, process, express, or defuse it. I find this is particularly helpful for recurring nightmares on the same themes. One technique I stumbled upon a few years ago is to paint the scene from the nightmare that has the most emotional weight, the most intensity to it. I’ve found that if I get this out of my head and onto the page, I tend to stop having the nightmare. Here’s one of the milder examples of this type of painting.
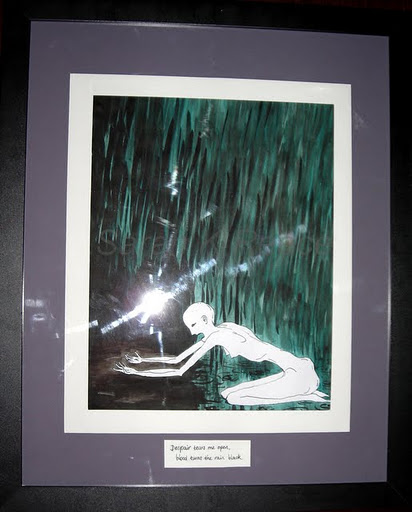
I didn’t need to look at the paintings or hang them anywhere. I found them profoundly disturbing and hated the sight of them. Once they were finished I would put them out of sight and only after a lot of time had passed would I take them out and have a look at them. I found just being able to get this feeling or fear or image out of my own head and safely recorded somewhere else was often enough to stop the nightmare.
For nightmares that aren’t recurring I find I need a different approach. There may be a common underlying theme, like being pursued, but the content of each nightmare is quite unique. In this case I find journalling is more useful. Sometimes I find words most useful to explore and express concepts and feelings, and other times visual images have more power for me. Sometimes I find that having written them, I can see themes and symbols more clearly in the content and make sense of what the underlying fears are. Here’s an example from my journal:
31 October 2007
I had one of my only reoccurring dreams – that the world was ending. I have these fairly frequently. They take different forms by the end of the world is always signalled by all the stars falling from the sky. Sometimes it is peaceful and beautiful, sometimes violent and terrifying, where the earth cracks open and monsters come out and devour everyone. Sometimes the stars take hours to all fall, sometimes they come down in a single storm of light, often there’s some kind of pattern, like all the stars falling in a perfect spiral, starting from the centre of the sky and moving down to those by the horizon. It always takes my breath away and fills me with such awe, such a sense of smallness and powerlessness. It’s the most beautiful thing I’ve ever seen.In this dream, the stars suddenly started to fall from a dark sky, like huge drops of bright rain, leaving only the black void behind them. But as they fell to earth, they suddenly took off in all directions. The truth is, they were enemy spaceships, all this time, and now they are attacking. I call to my crew and launch my spaceship to fight them but I do so with cold despair because I know there are far too many of them and we are doomed to be destroyed. I am so sad and shocked that the stars we’ve always admired and dreamed about were really enemies, watching and waiting, all this time.
And then I wake… I am realising my dreams are not just an escape from reality, but also a form of communication inside me. I’m not too concerned about what they mean so much as letting myself know I accept them. I’m listening. The dreams about the end of the world might seem to be obviously about fear but I think they’re about destruction as much as change. This is not the end of everything, in the dreams, it is the end of everything I have ever known, of how things have always been… Sometimes this transition is peaceful and sometimes it is violent and terrifying, but it’s always frightening, inevitable, and out of my control.
In this case, this was the last dream I have had so far about the end of the world. The dreams progressed until this final one where the stars were revealed to be enemies, and I’ve never had them again. I had worked through and communicated to myself what I needed to. Journaling can be a powerful way to record and contemplate dreams and nightmares.Developing the capacity to lucid dream may also help you to engage with your nightmares in a productive way. There are some suggestions about how to develop the capacity to lucid dream here. Simply put, lucid dreaming is being able to be aware that you are having a dream while you’re in it, and then to change and affect the dream. Personally I don’t find this so useful. I can lucid dream (not always) but I find that my nightmares adapt to my attempts to control them and my subconscious is far more powerful than I am when it comes to changing a dream. If I can create bridges to escape on, my mind can set them on fire. If I can imagine a safe place to hide in, it floods with black water and drowns me. I am not afraid of being physically harmed, but the psychological stress and trauma that come with living through these mock executions is massive. In some of my worst nightmares terrible things happen to me while I desperately try to scream myself awake or cause myself sufficient pain to wake me and it does not work. But for other people, being able to tell the difference between a dream and real life dramatically reduces their distress and may open the way for many other creative options in engaging a nightmare.
Engaging the content of the dream like this can also be done in real life. If you have painted a nightmare, you can respond to that painting with something that is meaningful and comforting to you. Paint in wings to carry you to safety, a sword or lion to protect you, whatever fits and feels right. You can write the dream out and then rewrite the ending in a way that fits. You can treat these re-visioning of your dreams as a way to talk back to your subconscious and tell it what would happen this time if you were in that kind of terrible situation. If you can make yourself feel heard and then engage with the distress, your mind may stop bringing up the nightmares.
Sometimes dreams speak to us of things we have deeply buried. This suppressed material – memories, knowledge, feelings, fears, hopes, can torment us at night when we cannot keep it contained. Sometimes it is not writing about the nightmares that helps, but writing about the memory or fear or aspect of ourselves we hate that helps. Being able to accept the reality of these things instead of fighting and suppressing them can reduce nightmares about them.
Reducing the Impact
In a completely different approach, these strategies are all about reducing your focus on the nightmares and reducing their power to affect you. For example, if you wake following a nightmare, instead of journalling and contemplating it, get straight out of bed, put on some music, make breakfast, engage in other distracting activities before the dream has settled into your memory. Creating a good bedroom space can greatly diminish the distress that nightmares cause. It needs to be a space that is safe and comfortable. Clutter, frightening pictures or shadows, tangling in bedclothes and sheets can all increase the impact of nightmares. Since childhood I haven’t been able to sleep with a cupboard door open in the room. I experience mild stress-related hallucinations and following a nightmare if the wrong cues are around me I will hallucinate the nightmare content in that dazed state between dreaming and awake. Open cupboards for me are portals that things come through. If your bedroom is setting you off, you may need to sleep elsewhere during bad nightmare cycles. You may also find that some approaches that soothe many people with autism who get easily overloaded by sensory input may help you. An easy one to adapt to the bedroom is a weighted blanket. Many people (and most animals) find being gently but firmly held, or nestled under heavy blankets to be calming and reassuring. Another common one I use is white noise to help me tune out other sounds and stay asleep. You can buy devices like this one, or find your own. I like a fan running by my bed for the sound it makes. This site has many other suggestions and ideas for people who have difficult with sensory overload or crave extra sensory stimulation to help them feel calm.
Many people have a strong preference for sleeping with the lights on or off, follow your own even if you feel a bit silly. I cannot sleep with the lights on because then I feel exposed and vulnerable. Try playing music especially sleep inducing music at bedtime. This kind is designed to gently slow your heartbeat and relax you, it can help when you wake panicked too. Reduce your access to the kinds of things that increase your nightmares such as violent movies. Try adding in some neutral content immediately before sleeping so that your brain has something else to form dreams about instead of your own subconscious. I always read in bed before going to sleep, always no matter what. This is essential to reduce the intensity and amount of the nightmares that I have. It doesn’t stop them but it dials them down a bit. Don’t stay up late working, studying, doing housework or arguing. Make sure the bedtime routine has wind-down time in it, a bath, episode of Blackadder, massage, whatever you find relaxing. Grounding techniques can help a lot before sleep or when waking up from nightmares. Consider sleeping with someone else in the bed or nearby to soothe you, or with a companion of some kind. I have a big hairy toy dog. A pet can also be an incredibly non-judgmental and nurturing companion in the night for those of us prone to waking up screaming and distressed.
If you are waking other people up by screaming or struggling, you can quickly get into a miserable feedback loop where you feel so embarrassed or anxious about the effect you’re having on them that your stress level increases and the nightmares get worse. This especially applies if you have young children in the house who are getting scared. Talk to them about what is going on, let them comfort you, and look after yourself. Any general stress reduction techniques that work for you are a good idea, do more of all of them for yourself and anyone else in your house. You need extra time having fun together in these kinds of situations.
You may want to seek counselling or therapy of some kind if you’re having a lot of trouble with nightmares. PTSD is very responsive to good therapy, hypnosis can be very useful, and good emotional support can make a big difference. I hope you’ve found some useful suggestions in these posts. There are some more ideas about managing nightmares here, and there are many books and websites on the topic. If you’re struggling or my strategies aren’t working very well for you, go have a look at what other people are finding effective and hopefully you’ll come across some ideas that make a difference. Good luck.